

초록접수 현황
| 20F-194 | 구연 발표 |
The Role of False Lumen Area Ratio on Late Aortic Events after Open Repair of Non-Syndromic Acute Type I Aortic Dissection
Jung-Hwan Kim, Seung Hyun Lee, Sak Lee, Young-Nam Youn, Kyung-Jong Yoo, Hyun-Chel Joo
Division of Cardiovascular Surgery, Department of Thoracic and Cardiovascular Surgery, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea
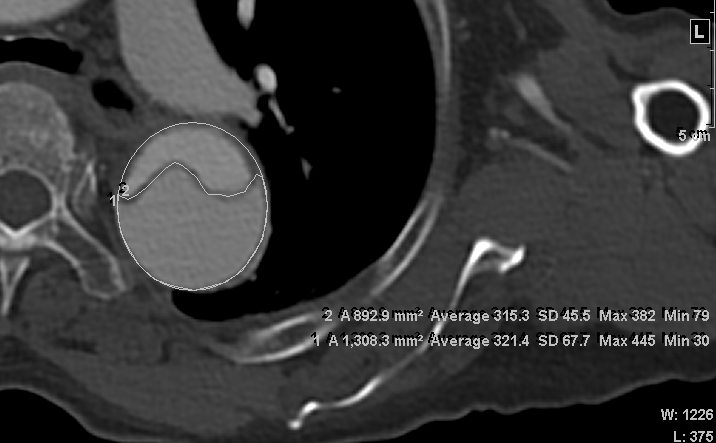
Purpose : The aim of this study was to determine whether distal aortic maximum false lumen area (MFLA) ratio predicts the late aortic dilatation and reintervention after open repair of acute type I aortic dissection.
Methods : We analyzed 309 non-syndromic acute type I aortic dissection patients, who were treated with a repair to the proximal aorta between 1994 and 2017. From 230 patients who did not show completely thrombosed false lumen on post-operative computed tomography (CT), MFLA ratio (MFLA/aortic area) on descending thoracic or abdominal aorta was measured with post-operative CT. The patients were divided into 3 groups according to the quartile range of MFLA ratio: low (<0.62, n=57), intermedius (0.62-0.81, n=116), and high (≥0.82, n=57) MFLA group.
Results : The 10-year freedom from aortic reintervention rate was significantly lower in high MFLA group (37.4±7.6%) compared with low (97.9±2.1%, p<0.01) and intermedius (91.0±3.4%, p<0.01) MFLA group. The aortic expansion rate was significantly higher in high MFLA group (11.5±21.2mm/year) compared with low (1.1±7.6mm/year, p<0.01) and intermedius (3.6±7.6mm/year, p=0.02) MFLA group. The 10-year freedom from significant aortic expansion rate was significantly lower in high MFLA group (33.5±7.9%) compared with low (97.6±2.4%, p<0.01) and intermedius (73.9±6.6%, p<0.01) MFLA group. The multivariate analysis showed that a high MFLA was an independent risk factor for aorta reintervention (HR=5.84, 95% CI=2.35-14.50, p<0.01) and significant aortic expansion (HR=2.22, 95% CI=1.15-4.30. p=0.02).
Conclusion : A high MFLA ratio on descending thoracic or abdominal aorta after acute type I aortic dissection repair was associated with increased the risk of late aortic reintervention and distal aortic dilatation.
Methods : We analyzed 309 non-syndromic acute type I aortic dissection patients, who were treated with a repair to the proximal aorta between 1994 and 2017. From 230 patients who did not show completely thrombosed false lumen on post-operative computed tomography (CT), MFLA ratio (MFLA/aortic area) on descending thoracic or abdominal aorta was measured with post-operative CT. The patients were divided into 3 groups according to the quartile range of MFLA ratio: low (<0.62, n=57), intermedius (0.62-0.81, n=116), and high (≥0.82, n=57) MFLA group.
Results : The 10-year freedom from aortic reintervention rate was significantly lower in high MFLA group (37.4±7.6%) compared with low (97.9±2.1%, p<0.01) and intermedius (91.0±3.4%, p<0.01) MFLA group. The aortic expansion rate was significantly higher in high MFLA group (11.5±21.2mm/year) compared with low (1.1±7.6mm/year, p<0.01) and intermedius (3.6±7.6mm/year, p=0.02) MFLA group. The 10-year freedom from significant aortic expansion rate was significantly lower in high MFLA group (33.5±7.9%) compared with low (97.6±2.4%, p<0.01) and intermedius (73.9±6.6%, p<0.01) MFLA group. The multivariate analysis showed that a high MFLA was an independent risk factor for aorta reintervention (HR=5.84, 95% CI=2.35-14.50, p<0.01) and significant aortic expansion (HR=2.22, 95% CI=1.15-4.30. p=0.02).
Conclusion : A high MFLA ratio on descending thoracic or abdominal aorta after acute type I aortic dissection repair was associated with increased the risk of late aortic reintervention and distal aortic dilatation.
책임저자: Hyun-Chel Joo
Division of Cardiovascular Surgery, Department of Thoracic and Cardiovascular Surgery, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea
발표자: Jung-Hwan Kim, E-mail : jhkim0907@yuhs.ac