

초록접수 현황
| 20F-066 | 구연 발표 |
The Fate of Aortic Arch in Patients with Invisible Tear during Acute Type A Aortic Dissection Repair
Wan Kee Kim, MD (1), Tae-Hoon Kim, MD (2), Seung Jun Song, MD, PhD (1), Hye Sun Lee, PhD (3), Suk-Won Song, MD, PhD (2)
(1) Department of Cardiothoracic Surgery, Yonsei University Medical Center, Yongin, Gyeonggi-do, South Korea
(2) Department of Cardiovascular Surgery, Gangnam Severance Hospital, Seoul, Republic
of Korea
(3) Biostatistics Collaboration Unit, Yonsei University College of Medicine, Seoul, Republic
of Korea
Purpose : Decision whether to repair the arch during acute aortic dissection (AD) repair has been conundrum when the macroscopic intimal tear is invisible during the surgery.
Methods : Using the institutional database from 2008 to 2018, we retrieved 71 patients (60.0±13.2 years; 42.3% females) who underwent non-total arch replacements for acute retrograde type A AD or intramural hematoma. The primary outcome was set for postoperative arch expansion over 5mm/year. To determine predictive factors for the arch expansion, a multivariable risk analysis was performed. The secondary outcome was a composite of intervention, surgery or rupture of the arch. For benchmark comparison, patients undergoing total arch replacement during same study period were reviewed (n=36).
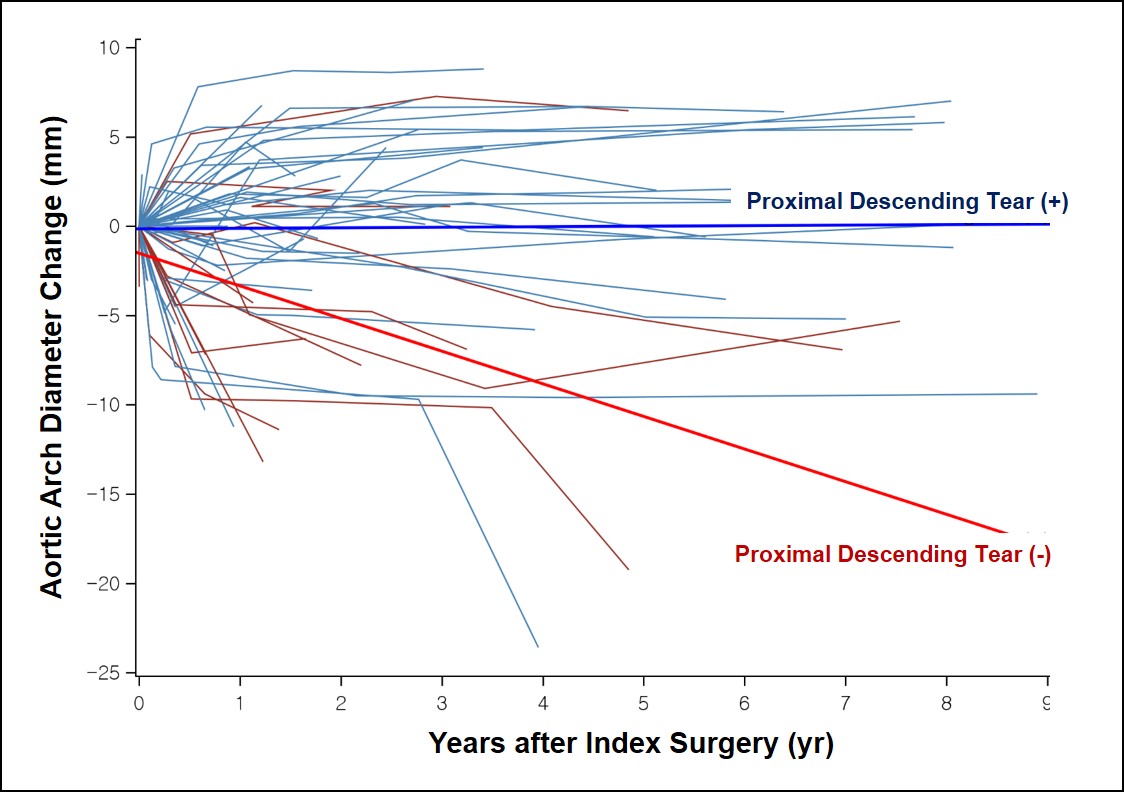
Results : The mean of baseline maximal arch diameter was 36.5±3.8 mm. During median follow-up of 46.5 (interquartile range, 12.9-94.4) months, a significant arch expansion was detected in 22 (31.0%) patients. On multivariable risk analyses, the presence of intimal tear in the proximal descending aorta (HR 1.36, 95%CI 1.06-1.76, p=0.02) and in the arch vessels (HR 1.39, 95%CI 1.02-1.89, p=0.04) emerged as independent factors for the significant arch expansion. Estimated yearly expansion rates were 0.03±0.23mm/year and -1.83±0.45mm/year in patients with and without proximal descending tear, respectively (Figure, p<0.001). Among overall 71 patients, 13 (5.39%/ patient-years) secondary outcomes occurred. Meanwhile, three (8.4%) early adverse events were observed in patients with initial total arch replacement.
Conclusion : Even in cases of invisible tear during acute type A AD repair, the postoperative arch expansion and requirements for re-intervention were frequent.
Methods : Using the institutional database from 2008 to 2018, we retrieved 71 patients (60.0±13.2 years; 42.3% females) who underwent non-total arch replacements for acute retrograde type A AD or intramural hematoma. The primary outcome was set for postoperative arch expansion over 5mm/year. To determine predictive factors for the arch expansion, a multivariable risk analysis was performed. The secondary outcome was a composite of intervention, surgery or rupture of the arch. For benchmark comparison, patients undergoing total arch replacement during same study period were reviewed (n=36).
Results : The mean of baseline maximal arch diameter was 36.5±3.8 mm. During median follow-up of 46.5 (interquartile range, 12.9-94.4) months, a significant arch expansion was detected in 22 (31.0%) patients. On multivariable risk analyses, the presence of intimal tear in the proximal descending aorta (HR 1.36, 95%CI 1.06-1.76, p=0.02) and in the arch vessels (HR 1.39, 95%CI 1.02-1.89, p=0.04) emerged as independent factors for the significant arch expansion. Estimated yearly expansion rates were 0.03±0.23mm/year and -1.83±0.45mm/year in patients with and without proximal descending tear, respectively (Figure, p<0.001). Among overall 71 patients, 13 (5.39%/ patient-years) secondary outcomes occurred. Meanwhile, three (8.4%) early adverse events were observed in patients with initial total arch replacement.
Conclusion : Even in cases of invisible tear during acute type A AD repair, the postoperative arch expansion and requirements for re-intervention were frequent.
책임저자: Suk-Won Song
Department of Cardiovascular Surgery, Gangnam Severance Hospital, Seoul, Republic
발표자: Wan Kee Kim, E-mail : sgwkwhite@yonsei.ac