

초록접수 현황
| 20F-043 | 구연 발표 |
Emergency or Urgency : Golden Time for Treatment of Acute Type A Aortic Dissection
Tae-Hoon Kim1, Ha Lee1, Myeong su Kim1, Seung Jun Song2, Wan Kee Kim2, Suk-Won Song1, Kyung-Jong Yoo3
1 Department of Thoracic and Cardiovascular Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea
2 Department of Thoracic and Cardiovascular Surgery, Yongin Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea
3 Department of Thoracic and Cardiovascular Surgery, Cardiovascular Hospital, Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea
2 Department of Thoracic and Cardiovascular Surgery, Yongin Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea
3 Department of Thoracic and Cardiovascular Surgery, Cardiovascular Hospital, Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea
Purpose : The purpose of this study is to suggest which acute type A aortic dissection (ATAD) are emergency and demonstrate the golden time.
Methods : Between 2009 and 2020, 535 patients underwent emergent open aortic repair for type A aortic dissection. Of these, 518 patients with ATAD were reviewed. Impending cardiac tamponade was defined as pericardial effusion with reflux of contrast material into IVC, hepatic vein and/or azygos vein on imaging study. Preoperative neurologic deficit was defined as lateralizing sign and/or impaired consciousness with cerebral malperfusion sign on imaging study. Time interval from 'symptom to operation' and 'emergency room (ER) to operation' were reviewed. 30-day mortality and overall mortality were evaluated.
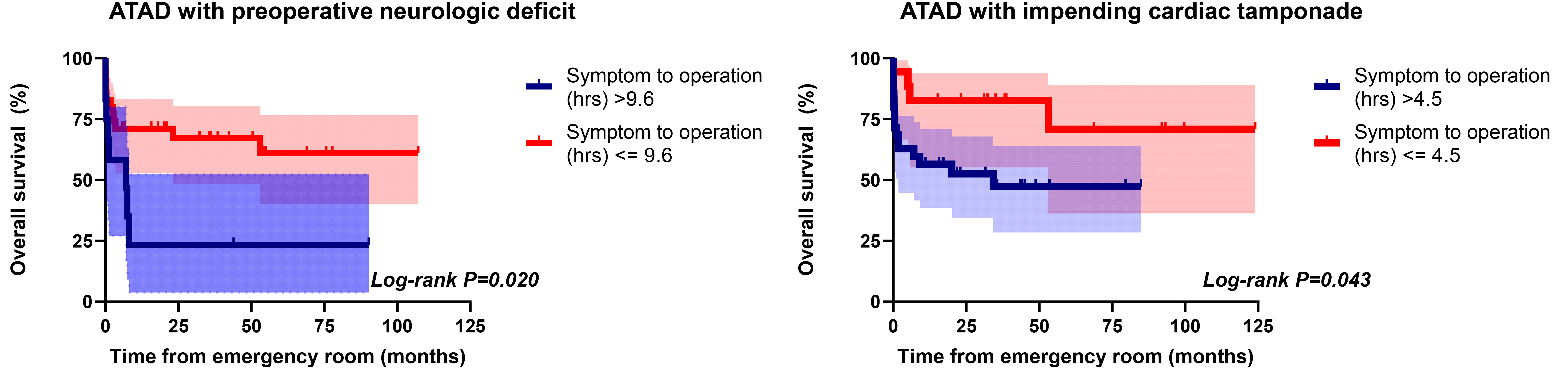
Results : Median follow-up duration was 30 months (IQR 7.1-76.8). Symptom to operation (hrs) and ER to operation (hrs) were 8.5 hrs (IQR 5.7-17.3) and 1.8 hrs (IQR 1.3-3.0), respectively. 30-day, in-hospital and overall mortality was 9.7%, 12.5% and 19.1%, respectively. Age (Hazards ratio [HR] 1.05, p<0.001), impending cardiac tamponade (HR 2.17, p=0.003), preoperative neurologic deficit (HR 1.84, p=0.025) and visceral malperfusion (HR 1.92, p=0.008) were independently significant risk factors for overall mortality. Cut-off values of symptom to operation (hrs) were 4.5 hrs for impending cardiac tamponade and 9.6 hrs for preoperative neurologic deficit, respectively (Figure).
Conclusion : ATAD is a devastating and emergent disease. However, not all ATAD is a time bomb because ATAD has a wide spectrum. In ATAD patients with impending cardiac tamponade and preoperative neurologic deficit, operation should be initiated within 4.5 hrs and 9.6 hrs, respectively.
Methods : Between 2009 and 2020, 535 patients underwent emergent open aortic repair for type A aortic dissection. Of these, 518 patients with ATAD were reviewed. Impending cardiac tamponade was defined as pericardial effusion with reflux of contrast material into IVC, hepatic vein and/or azygos vein on imaging study. Preoperative neurologic deficit was defined as lateralizing sign and/or impaired consciousness with cerebral malperfusion sign on imaging study. Time interval from 'symptom to operation' and 'emergency room (ER) to operation' were reviewed. 30-day mortality and overall mortality were evaluated.
Results : Median follow-up duration was 30 months (IQR 7.1-76.8). Symptom to operation (hrs) and ER to operation (hrs) were 8.5 hrs (IQR 5.7-17.3) and 1.8 hrs (IQR 1.3-3.0), respectively. 30-day, in-hospital and overall mortality was 9.7%, 12.5% and 19.1%, respectively. Age (Hazards ratio [HR] 1.05, p<0.001), impending cardiac tamponade (HR 2.17, p=0.003), preoperative neurologic deficit (HR 1.84, p=0.025) and visceral malperfusion (HR 1.92, p=0.008) were independently significant risk factors for overall mortality. Cut-off values of symptom to operation (hrs) were 4.5 hrs for impending cardiac tamponade and 9.6 hrs for preoperative neurologic deficit, respectively (Figure).
Conclusion : ATAD is a devastating and emergent disease. However, not all ATAD is a time bomb because ATAD has a wide spectrum. In ATAD patients with impending cardiac tamponade and preoperative neurologic deficit, operation should be initiated within 4.5 hrs and 9.6 hrs, respectively.
책임저자: Suk-Won Song
Department of Thoracic and Cardiovascular Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea
발표자: Tae-Hoon Kim, E-mail : airtech2@yuhs.ac