



초록접수 현황
| 19F-241 | 포스터 발표 |
Giant Bullae Mistaken for Tension Pneumothorax
Se Min Ryu, Kyung-Hak Lee, Sung-Min Park, Seong-Joon Cho, Han Pil Lee, Se-Ran Yang, Ki Hwan Kim, Jung Eui Yun, Jin Soo Lee, Hye Jin Park, Young Heon Park, Jooyeon Lee, Hanbyeol Lee
Department of Thoracic and Cardiovascular Surgery, Kangwon National University Hospital, Kangwon National University College of Medicine, Gangwon-do, Republic of Korea
Purpose : Giant bullae and tension pneumothorax can produce similar signs and radiological appearances. The differential diagnosis between giant bullae and tension pneumothorax is thought to be straightforward but sometimes poses a challenge. This case report demonstrates the clinical presentation of giant bullae and its complications such as pneumothorax and also highlights the difficulty in making this diagnosis and appropriately treating it.
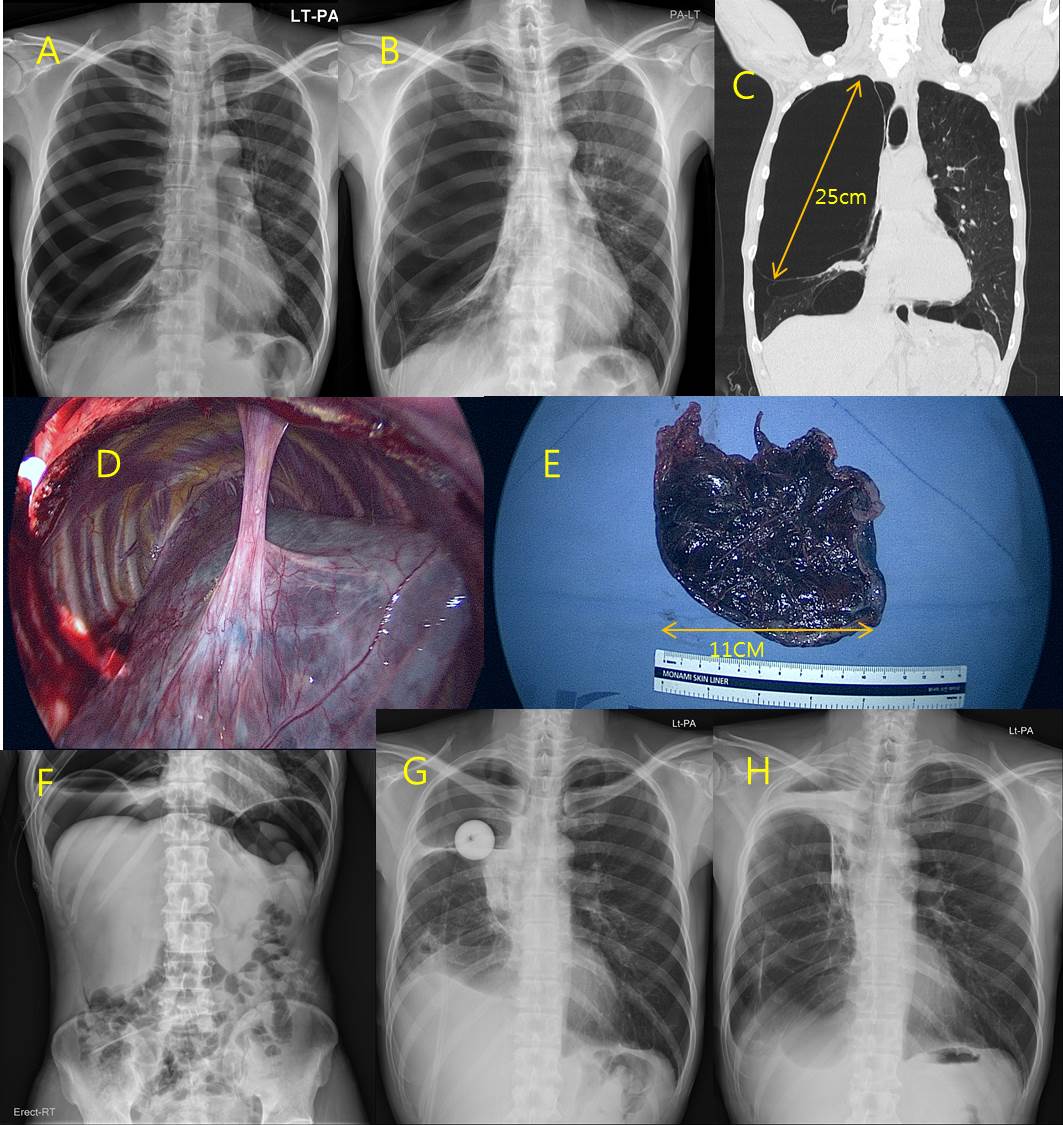
Methods : A 47 years old male chronic smoker was admitted with respiratory distress having history of gradually progressive dyspnea since 3 weeks with productive cough. Chest X-ray showed large lucent areas over the entire right thorax with mediastinal shift to left (Figure A). A Chest tube was inserted under the diagnosis of tension pneumothorax. Follow-up chest radiography showed little expansion of the right lung but restored mediastinum (Figure B). Computed tomography of chest subsequently demonstrated giant bullae occupying the entire right thorax with right lung compressive atelectasis and remnant pneumothorax (Figure C).
Results : The patient underwent bullectomy of right giant bullae by right thoracotomy (Figure D, E). Postoperative air leak was noted and treated with talc pleurodesis, artificial pneumoperitoneum (Figure F) and another closed thoracostomy using foley catheter (Figure G). The patient was in stable condition after 6 month of follow-up (Figure H).
Conclusion : Giant bullae and tension pneumothorax should be differentiated in detail when chest radiography in a smoker presents with large lucent areas. We recommend that in cases where pneumothorax is suspected, if the patient is clinically stable, imaging studies including computed tomography should be performed prior to closed thoracostomy.
Methods : A 47 years old male chronic smoker was admitted with respiratory distress having history of gradually progressive dyspnea since 3 weeks with productive cough. Chest X-ray showed large lucent areas over the entire right thorax with mediastinal shift to left (Figure A). A Chest tube was inserted under the diagnosis of tension pneumothorax. Follow-up chest radiography showed little expansion of the right lung but restored mediastinum (Figure B). Computed tomography of chest subsequently demonstrated giant bullae occupying the entire right thorax with right lung compressive atelectasis and remnant pneumothorax (Figure C).
Results : The patient underwent bullectomy of right giant bullae by right thoracotomy (Figure D, E). Postoperative air leak was noted and treated with talc pleurodesis, artificial pneumoperitoneum (Figure F) and another closed thoracostomy using foley catheter (Figure G). The patient was in stable condition after 6 month of follow-up (Figure H).
Conclusion : Giant bullae and tension pneumothorax should be differentiated in detail when chest radiography in a smoker presents with large lucent areas. We recommend that in cases where pneumothorax is suspected, if the patient is clinically stable, imaging studies including computed tomography should be performed prior to closed thoracostomy.
책임저자: Se Min Ryu
Department of Thoracic and Cardiovascular Surgery, Kangwon National University Hospital, Kangwon National University College of Medicine, Gangwon-do, Republic of Korea
발표자: Se Min Ryu, E-mail : semin@kangwon.ac.kr