



초록접수 현황
| 19F-008 | 구연 발표 |
Three-dimensional Totally Endoscopic Reoperative Mitral Valve Surgery with Fibrillatory Arrest (Aortic No-touch Technique)
Jae Suk Yoo, Wan Kee Kim, Sang Yoon Yeom, Hee Moon Lee, Dong Jin Kim, Kwang Ree Cho
Department of Thoracic and Cardiovascular Surgery, Sejong General Hospital, Gyeonggi-do, Republic of Korea
Purpose : In mitral valve(MV) surgery after previous sternotomy, right minithoracotomy and fibrillatory arrest(FA) offers the simplest approach with no need for mediastinal adhesiolysis. Despite this advantage, limited dissection and fibrillating heart sometimes yields limited exposure. A three-dimensional(3D) endoscope might facilitate to visualize and manipulate the MV, which enables totally endoscopic surgery. We present the earliest experience of applying 3D endoscopic system in redo MV surgery with FA.
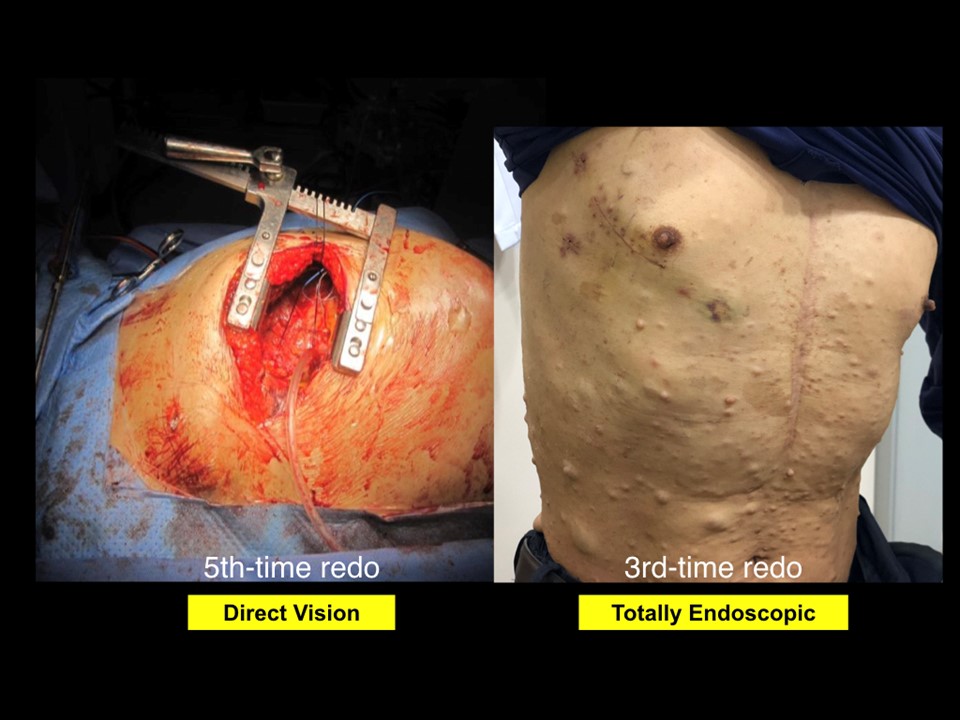
Methods : Between May 2018 and June 2019, we performed aortic no-touch totally endoscopic redo mitral valve surgery on 25 patients; second-time in 19 patients, third-time in three patients, fourth-time in three patients. All patients had undergone previous valve surgeries involving mitral valves only through sternotomy approach (EuroScore II 12.92±10.64%). Previously implanted prosthetic aortic valves existed in nine patients. All procedures were performed through 5-6cm right minithoracotomy incision with two extra ports; a left atrial sump drain and a 10 mm-scope trocar (Frigure, Right). Left atrium was opened after inducing FA with a fibrillator.
Results : Mean cardiopulmonary bypass time was 186.1±33.4 minutes. No intraoperative events such as great vessel injury or lung laceration occurred. There were no perioperative mortality, postoperative bleeding reoperation, pneumonia, or wound problem. One major stroke occurred in a patient with fourth-time redo mitral valve replacement. One intraoperative conversion to clamshell incision was required. Concomitant procedures including tricuspid valvuloplasty in 18 and maze procedure in four were performed.
Conclusion : Our experience illustrates feasibility and safety of the 3D totally endoscopic right minithoracotomy approach under FA to treat mitral pathology without reoperative sternotomy risks.
Methods : Between May 2018 and June 2019, we performed aortic no-touch totally endoscopic redo mitral valve surgery on 25 patients; second-time in 19 patients, third-time in three patients, fourth-time in three patients. All patients had undergone previous valve surgeries involving mitral valves only through sternotomy approach (EuroScore II 12.92±10.64%). Previously implanted prosthetic aortic valves existed in nine patients. All procedures were performed through 5-6cm right minithoracotomy incision with two extra ports; a left atrial sump drain and a 10 mm-scope trocar (Frigure, Right). Left atrium was opened after inducing FA with a fibrillator.
Results : Mean cardiopulmonary bypass time was 186.1±33.4 minutes. No intraoperative events such as great vessel injury or lung laceration occurred. There were no perioperative mortality, postoperative bleeding reoperation, pneumonia, or wound problem. One major stroke occurred in a patient with fourth-time redo mitral valve replacement. One intraoperative conversion to clamshell incision was required. Concomitant procedures including tricuspid valvuloplasty in 18 and maze procedure in four were performed.
Conclusion : Our experience illustrates feasibility and safety of the 3D totally endoscopic right minithoracotomy approach under FA to treat mitral pathology without reoperative sternotomy risks.
책임저자: Jae Suk Yoo
Department of Thoracic and Cardiovascular Surgery, Sejong General Hospital, Gyeonggi-do, Republic of Korea
발표자: Jae Suk Yoo, E-mail : mdyoo77@gmail.com