













초록접수 현황
| 15F-078 | 구연 발표 |
Double Inlet Left Ventricle or Tricuspid Atresia with Transposition of the Great Arteries: Impact of Initial Arch Obstruction on the Need for Systemic Outflow Relief Procedure
박원균¹, 방지현¹, 박천수¹, 박정준¹, 구현우², 백재숙³, 유정진³, 김영휘³, 고재곤³, 윤태진¹
울산대학교 의과대학 서울아산병원 흉부외과학교실 소아심장외과¹, 울산대학교 의과대학 서울아산병원 영상의학과학교실², 울산대학교 의과대학 서울아산병원 소아과학교실 소아심장과³
목적 : Patients with double inlet left ventricle (DILV) or tricuspid atresia (TA) with transposition of the great arteries (TGA) tend to develop systemic outflow tract obstruction in the course of Fontan palliation, especially when arch obstruction is associated.
방법 : Between June 1989 and June 2015, 44 patients (M: F= 29:15) with DILV with TGA or TA (IIc) underwent various procedures for single ventricle palliation. Arch obstruction (AO) was associated in 14 patients: Discrete coarctation of the aorta (CoA) or aortic arch hypoplasia in 9, interrupted aortic arch (IAA) in 5. Various systemic outflow relief operations (SORO), including Damus-Kaye-Stansel (DKS) procedure (n=10), Norwood operation (n=2), palliative arterial switch operation (n= 2), internal pulmonary banding with aortopulmonary window formation (n=2), ventriclular septal defect (VSD) widening (n= 4), were performed as a initial palliation (n= 8), upon bidirectional cavopulmonary shunt (BCS) (n= 10), and upon the Fontan procedure (n=2).
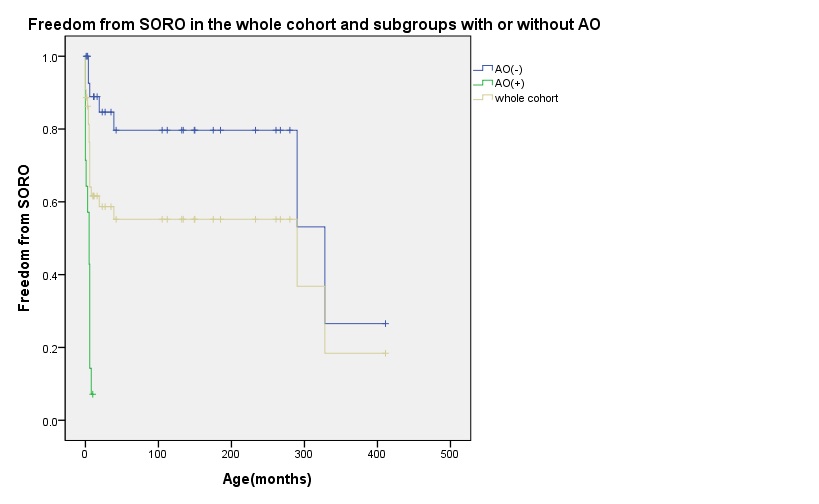
결과 : There were eight deaths (five after the 1st palliation, one after BCS, and two after the Fontan operation) and five follow-up loss. Currently 21 patients are post-Fontan state, eight patients are waiting for the Fontan procedure after BCS, and two patients are waiting for BCS after the initial palliation. SORO was required in 20 patients (13/14 with AO, 7/30 without AO) during the course of the Fontan track. Freedom from SORO at 1 year was 61.6 ± 7.6% (7.1% ± 6.9 in patients with AO, 84.7% ± 7.1% in patients without AO, inter-group difference by log-rank test: P<0.001). On Cox proportional hazards modeling, AO was identified as a risk factor for SORO (HR, 22.07 (95% CI 6.11-79.7), p<0.01).
결론 : In patients with DILV with TGA with TA (IIc), SORO was eventually required in the majority of the patients during the course of Fontan palliation, especially when AO was initially combined. Therefore, even in patients without SORO at initial palliation, systemic outflow tract dimension should be carefully evaluated, especially when CoA or IAA was initially associated.
방법 : Between June 1989 and June 2015, 44 patients (M: F= 29:15) with DILV with TGA or TA (IIc) underwent various procedures for single ventricle palliation. Arch obstruction (AO) was associated in 14 patients: Discrete coarctation of the aorta (CoA) or aortic arch hypoplasia in 9, interrupted aortic arch (IAA) in 5. Various systemic outflow relief operations (SORO), including Damus-Kaye-Stansel (DKS) procedure (n=10), Norwood operation (n=2), palliative arterial switch operation (n= 2), internal pulmonary banding with aortopulmonary window formation (n=2), ventriclular septal defect (VSD) widening (n= 4), were performed as a initial palliation (n= 8), upon bidirectional cavopulmonary shunt (BCS) (n= 10), and upon the Fontan procedure (n=2).
결과 : There were eight deaths (five after the 1st palliation, one after BCS, and two after the Fontan operation) and five follow-up loss. Currently 21 patients are post-Fontan state, eight patients are waiting for the Fontan procedure after BCS, and two patients are waiting for BCS after the initial palliation. SORO was required in 20 patients (13/14 with AO, 7/30 without AO) during the course of the Fontan track. Freedom from SORO at 1 year was 61.6 ± 7.6% (7.1% ± 6.9 in patients with AO, 84.7% ± 7.1% in patients without AO, inter-group difference by log-rank test: P<0.001). On Cox proportional hazards modeling, AO was identified as a risk factor for SORO (HR, 22.07 (95% CI 6.11-79.7), p<0.01).
결론 : In patients with DILV with TGA with TA (IIc), SORO was eventually required in the majority of the patients during the course of Fontan palliation, especially when AO was initially combined. Therefore, even in patients without SORO at initial palliation, systemic outflow tract dimension should be carefully evaluated, especially when CoA or IAA was initially associated.
책임저자: 윤태진
울산대학교 의과대학 서울아산병원 흉부외과학교실 소아심장외과
연락처 : 박원균, Tel: 02-3010-3575 , E-mail : medkyoun@naver.com
