










초록접수 현황
| 14F-019 | 구연 발표 |
Outcomes of Repeat Pulmonary Valve Replacement for Bioprosthetic Pulmonary Valve Failure in 61 Patients with Congenital Heart Disease
이철¹, 이창하², 곽재건²
가톨릭대학교 서울성모병원 흉부외과학교실¹, 세종병원 흉부외과²
Background : Although all bioprostheses used for pulmonary valve replacement (PVR) are prone to failure and will require repeat PVR, data pertaining to the outcomes of this procedure are lacking. The objective of this study was to evaluate outcomes of repeat PVR for bioprosthetic pulmonary valve (PV) failure in patients with congenital heart disease.
Methods : A retrospective review of 61 patients who underwent repeat PVR for bioprosthetic PV failure between November 1999 and June 2013 was performed. Univariable analyses were used to identify the factors associated with postoperative adverse events (PAE). Time-related events were analyzed using Kaplan-Meier method.
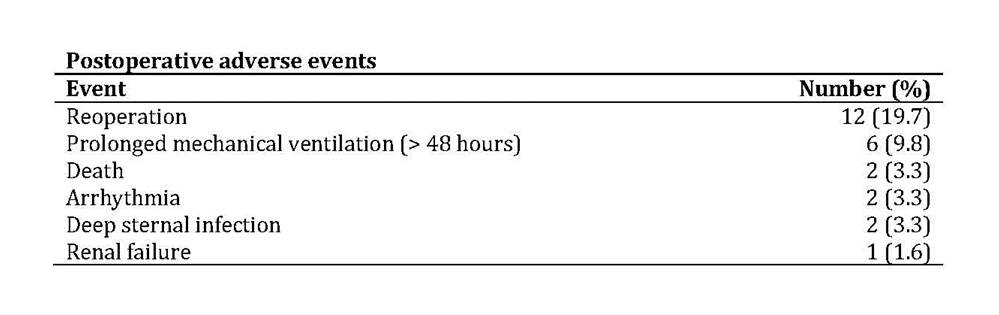
Results : The median age at initial PVR was 7.0 years (range, 1.6-36.5 years) and the median age at repeat PVR was 13.5 years (range, 7.6-43.3 years). Fundamental diagnoses were tetralogy of Fallot (n = 20), pulmonary atresia with ventricular septal defect (n = 20), double outlet right ventricle (n = 7), and others (n = 14). Indications for repeat PVR were pulmonary stenosis (PS, n = 36), combined PS and pulmonary regurgitation (n = 17), and infective endocarditis (n = 8). The median number of previous sternotomies was 2 (range, 1-4). At repeat PVR, reentry injury occurred in 2 patients (3.3%). The median valve size was 25 mm (range, 18-28 mm). Concomitant procedures were performed in 32 patients (52.5%). There were 2 early deaths (90-day hospital mortality, 3.3%) due to sepsis and brain injury. Eighteen patients (29.5%) experienced PAE (Table). The median duration of intensive care unit and hospital stay was 2 days (range, 1-10 days) and 15 days (range, 5-86 days), respectively. Thirty patients (50.8%) experienced prolonged (more than 14 days) hospital stay. PAE were associated with higher preoperative right ventricular (RV) systolic pressure (105 ± 22 mm Hg vs 89 ± 19 mmHg, P = .016) and longer bypass time (219 ± 77 minutes vs 164 ± 59 minutes, P = .007). Follow-up completeness was 95.8% and the median duration of follow-up was 5.5 years (range, 0.1-14.3 years). There were 3 late deaths. Actuarial survival at 5 and 10 years was 94.8 ± 2.9% and 83.7 ± 8.0%, respectively. Eleven patients underwent the second repeat PVR during follow-up. Freedom from the second repeat PVR at 5 and 10 years was 94.5 ± 3.1% and 58.8 ± 11.9%, respectively. Fifty-seven patients (96.6%) underwent follow-up echocardiography and the median interval to the latest echocardiographic examination was 4.5 years (range, 6 days-12.1 years). Freedom from both PV reintervention and structural valve deterioration (SVD) at 5 and 10 years was 89.2 ± 4.7% and 32.0 ± 13.3%, respectively.
Conclusion : A substantial number of the patients experienced mortality or morbidities after repeat PVR. Higher preoperative RV systolic pressure and longer bypass time were associated with PAE. By 10 years after the repeat PVR, approximately two thirds will require PV reintervention or manifest SVD.
Methods : A retrospective review of 61 patients who underwent repeat PVR for bioprosthetic PV failure between November 1999 and June 2013 was performed. Univariable analyses were used to identify the factors associated with postoperative adverse events (PAE). Time-related events were analyzed using Kaplan-Meier method.
Results : The median age at initial PVR was 7.0 years (range, 1.6-36.5 years) and the median age at repeat PVR was 13.5 years (range, 7.6-43.3 years). Fundamental diagnoses were tetralogy of Fallot (n = 20), pulmonary atresia with ventricular septal defect (n = 20), double outlet right ventricle (n = 7), and others (n = 14). Indications for repeat PVR were pulmonary stenosis (PS, n = 36), combined PS and pulmonary regurgitation (n = 17), and infective endocarditis (n = 8). The median number of previous sternotomies was 2 (range, 1-4). At repeat PVR, reentry injury occurred in 2 patients (3.3%). The median valve size was 25 mm (range, 18-28 mm). Concomitant procedures were performed in 32 patients (52.5%). There were 2 early deaths (90-day hospital mortality, 3.3%) due to sepsis and brain injury. Eighteen patients (29.5%) experienced PAE (Table). The median duration of intensive care unit and hospital stay was 2 days (range, 1-10 days) and 15 days (range, 5-86 days), respectively. Thirty patients (50.8%) experienced prolonged (more than 14 days) hospital stay. PAE were associated with higher preoperative right ventricular (RV) systolic pressure (105 ± 22 mm Hg vs 89 ± 19 mmHg, P = .016) and longer bypass time (219 ± 77 minutes vs 164 ± 59 minutes, P = .007). Follow-up completeness was 95.8% and the median duration of follow-up was 5.5 years (range, 0.1-14.3 years). There were 3 late deaths. Actuarial survival at 5 and 10 years was 94.8 ± 2.9% and 83.7 ± 8.0%, respectively. Eleven patients underwent the second repeat PVR during follow-up. Freedom from the second repeat PVR at 5 and 10 years was 94.5 ± 3.1% and 58.8 ± 11.9%, respectively. Fifty-seven patients (96.6%) underwent follow-up echocardiography and the median interval to the latest echocardiographic examination was 4.5 years (range, 6 days-12.1 years). Freedom from both PV reintervention and structural valve deterioration (SVD) at 5 and 10 years was 89.2 ± 4.7% and 32.0 ± 13.3%, respectively.
Conclusion : A substantial number of the patients experienced mortality or morbidities after repeat PVR. Higher preoperative RV systolic pressure and longer bypass time were associated with PAE. By 10 years after the repeat PVR, approximately two thirds will require PV reintervention or manifest SVD.
책임저자: 이철
가톨릭대학교 서울성모병원 흉부외과학교실
연락처 : 이철, Tel: 02-2258-6131 , E-mail : cheul@me.com
