










초록접수 현황
| 14F-162 | 포럼 발표 |
Comparison of Ventricular Volume Measured by Cardiac CT and MRI in Surgically Corrected TOF Patients
Ho Jin Kim¹; Chun Soo Park¹; Jeong-Jun Park¹; Hyun Woo Goo²; Tae-Jin Yun¹
Division of Pediatric Cardiac Surgery, Asan Medical Center, University of Ulsan College of Medicine¹
Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine²
Background : Cardiac MRI has been regarded as the gold standard for ventricular volumetry. However, long examination time and a requirement for general anesthesia have limited the use of MRI in pediatric patients with congenital heart disease, whereas cardiac CT has recently emerged as an alternative which can also provide more accurate structural information including coronary anatomy. We sought to evaluate the validity and reliability in ventricular volumetry by the use of cardiac CT.
Methods : By the review of our institutional prospective database, we identified 11 patients (mean age, 18.5 ± 4.2 years; 1 female) who had undergone total correction of tetralogy of Fallot (TOF) during infancy period, and undertook cardiac CT and MRI prior to pulmonary valve implantation (PVI). Right and left ventricular volumetry and cardiac function measured by both radiologic modalities were evaluated. Bland-Altman plots were used to assess the agreement between the two methods.
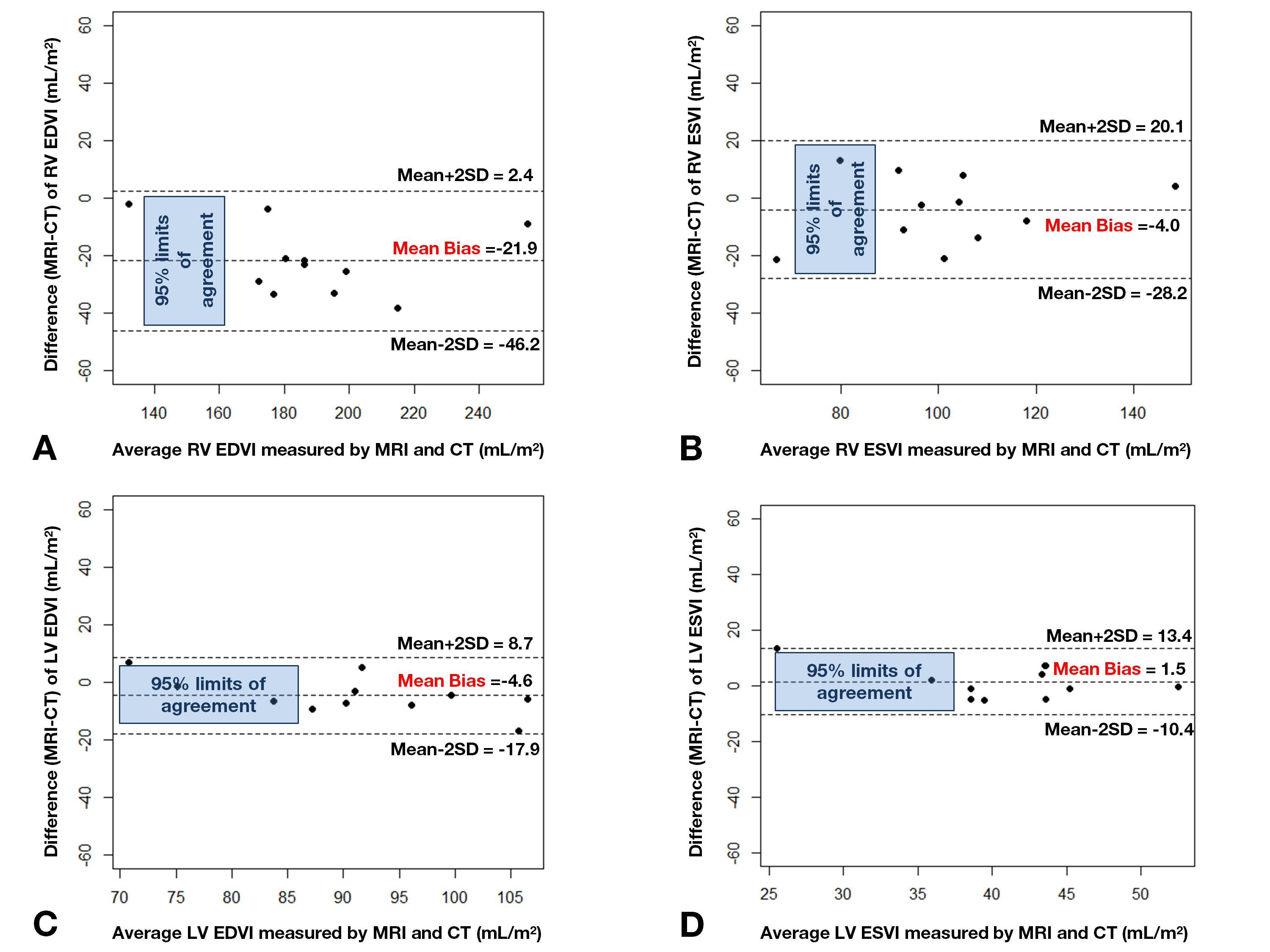
Results : Median interval between total correction of TOF and PVI was 213 months (Quartile 1-3, 190-250 months). Right ventricle end-diastolic (RVEDVI), end-systolic volume index (RVESVI), left ventricle end-diastolic (LVEDVI) and end-systolic volume index (LVESVI) measured by cardiac MRI were 177.6 ± 29.4, 99.2 ± 22.9, 88.4 ± 9.7, and 41.7 ± 6.1 mL/m2, respectively, whereas the same indices measured by cardiac CT were 199.5 ± 32.0, 103.2 ± 20.8, 93.0 ± 13.6, and 40.1 ± 8.4 mL/m2, respectively. The agreement between two imaging modalities, judged by Bland-Altman analysis (figure), showed that cardiac CT agrees well with MRI in terms of each volumetric index and cardiac function: RVEDVI (mean difference: range of 95% limits of agreement, -21.9: 2.4∼-46.2), RVESVI (-4.0: 20.1∼-28.1), LVEDVI (-4.6: 8.7∼-17.9), LVESVI (1.5: 13.4∼-10.4), RV ejection fraction (%) (-4.0: 9.7, -17.8), LVEF (%) (-3.62: 12.9, -20.1)
Conclusion : Ventricular volumetry tended to be underestimated with the use of cardiac MRI, which can be attributable to its low spatial resolution and the failure to capture the space between heavy trabeculation, especially in the RV. However, the biases measured by two imaging modalities were under clinical relevance. If CT is to be solely used for the preoperative assessment prior to PVI, RV volumetric criteria for PVI should be set higher than previously used MRI volumetric criteria.
Methods : By the review of our institutional prospective database, we identified 11 patients (mean age, 18.5 ± 4.2 years; 1 female) who had undergone total correction of tetralogy of Fallot (TOF) during infancy period, and undertook cardiac CT and MRI prior to pulmonary valve implantation (PVI). Right and left ventricular volumetry and cardiac function measured by both radiologic modalities were evaluated. Bland-Altman plots were used to assess the agreement between the two methods.
Results : Median interval between total correction of TOF and PVI was 213 months (Quartile 1-3, 190-250 months). Right ventricle end-diastolic (RVEDVI), end-systolic volume index (RVESVI), left ventricle end-diastolic (LVEDVI) and end-systolic volume index (LVESVI) measured by cardiac MRI were 177.6 ± 29.4, 99.2 ± 22.9, 88.4 ± 9.7, and 41.7 ± 6.1 mL/m2, respectively, whereas the same indices measured by cardiac CT were 199.5 ± 32.0, 103.2 ± 20.8, 93.0 ± 13.6, and 40.1 ± 8.4 mL/m2, respectively. The agreement between two imaging modalities, judged by Bland-Altman analysis (figure), showed that cardiac CT agrees well with MRI in terms of each volumetric index and cardiac function: RVEDVI (mean difference: range of 95% limits of agreement, -21.9: 2.4∼-46.2), RVESVI (-4.0: 20.1∼-28.1), LVEDVI (-4.6: 8.7∼-17.9), LVESVI (1.5: 13.4∼-10.4), RV ejection fraction (%) (-4.0: 9.7, -17.8), LVEF (%) (-3.62: 12.9, -20.1)
Conclusion : Ventricular volumetry tended to be underestimated with the use of cardiac MRI, which can be attributable to its low spatial resolution and the failure to capture the space between heavy trabeculation, especially in the RV. However, the biases measured by two imaging modalities were under clinical relevance. If CT is to be solely used for the preoperative assessment prior to PVI, RV volumetric criteria for PVI should be set higher than previously used MRI volumetric criteria.
책임저자: 윤태진
Division of Pediatric Cardiac Surgery, Asan Medical Center, University of Ulsan College of Medicine
연락처 : 김호진, Tel: 02-542-3224 , E-mail : rhonin.hojin@gmail.com
