










초록접수 현황
| 14F-010 | 구연 발표 |
Management of Acute Massive Pulmonary Embolism: Is Surgical Thrombectomy Inferior to Thrombolysis?
YANG HYUN CHO,* KIICK SUNG,* WOOK SUNG KIM,* DONG SEOP JEONG,*
YOUNG TAK LEE,* PYO WON PARK,* AND DUK-KYUNG KIM†
*Department of Thoracic and Cardiovascular Surgery, †Department of Internal Medicine, Division of Cardiology, Samsung Medical Center, Sungkyunkwan University School of Medicine
Background : According to the current guideline, the surgical embolectomy is only recommended when thrombolysis is contraindicated or failed. However, the clinical outcomes of thrombolysis and surgical thrombectomy have been rarely compared. Hence, we reviewed our experience.
Methods : We identified patients who had thrombolysis or surgical embolectomy for acute massive pulmonary embolism from 2000 to 2013 at Samsung Medical Center. Patients under 19 year-old or diagnosed as submassive or non-massive pulmonary embolism were excluded. The primary endpoint was cardiac mortality and secondary endpoints were early death and all-cause mortality.
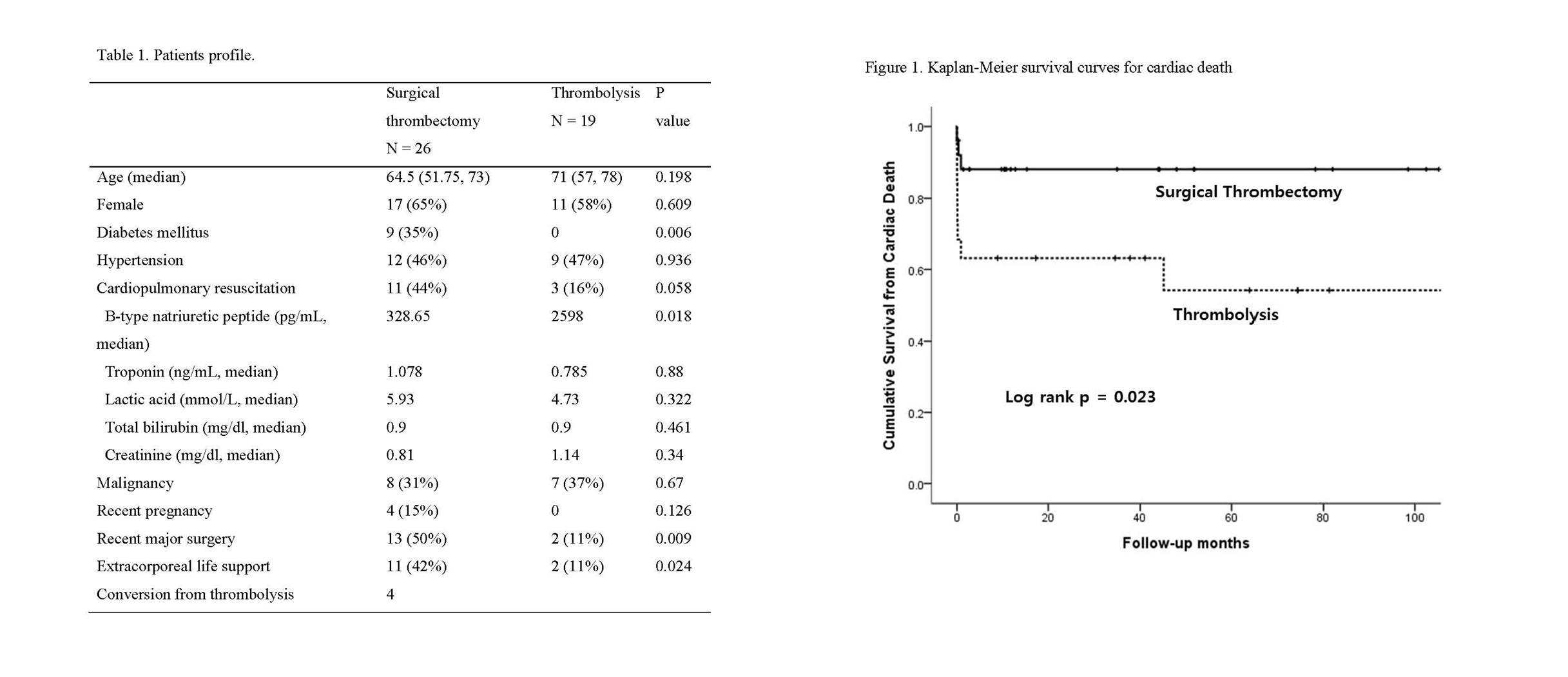
Results : Median overall follow-up duration was 17 months (range, 0 - 150). Of 45 patients enrolled, 26 had a surgical embolectomy and 19 had only thrombolysis. Four patients had surgery, because of failed thrombolysis. The median age was 68 (range, 21 – 86) and 28 (62%) were female. Fourteen patients (31%) had cardiac arrest before beginning of treatment for embolism. Fifteen patients (33%) had history of cancer diagnosis. Extracorporeal life support (ECLS) was used in 13 patients (29%). Comparison of patients characteristics are shown in Table 1. In surgical thrombectomy group, more patients had cardiac arrest and ECLS. Overall in-hospital mortality was 27%. (n = 12). Although there was no statistical significance, in-hospital mortality was high in thrombolysis group (37%) than thrombectomy group (19%). Cardiac mortality was significantly higher in the thrombolysis group than surgical thrombectomy group (log rank p = 0.023, Fig. 1), but all-cause death was not different (log rank p = 0.613). In multivariate analysis, thrombolysis was predictor of cardiac death.
Conclusion : In our experience, surgical thrombectomy was related to lower cardiac death than thrombolysis. For a patient who does not have life-limiting severe comorbidity, surgical thrombectomy can be a first-line option for acute massive pulmonary embolism.
Methods : We identified patients who had thrombolysis or surgical embolectomy for acute massive pulmonary embolism from 2000 to 2013 at Samsung Medical Center. Patients under 19 year-old or diagnosed as submassive or non-massive pulmonary embolism were excluded. The primary endpoint was cardiac mortality and secondary endpoints were early death and all-cause mortality.
Results : Median overall follow-up duration was 17 months (range, 0 - 150). Of 45 patients enrolled, 26 had a surgical embolectomy and 19 had only thrombolysis. Four patients had surgery, because of failed thrombolysis. The median age was 68 (range, 21 – 86) and 28 (62%) were female. Fourteen patients (31%) had cardiac arrest before beginning of treatment for embolism. Fifteen patients (33%) had history of cancer diagnosis. Extracorporeal life support (ECLS) was used in 13 patients (29%). Comparison of patients characteristics are shown in Table 1. In surgical thrombectomy group, more patients had cardiac arrest and ECLS. Overall in-hospital mortality was 27%. (n = 12). Although there was no statistical significance, in-hospital mortality was high in thrombolysis group (37%) than thrombectomy group (19%). Cardiac mortality was significantly higher in the thrombolysis group than surgical thrombectomy group (log rank p = 0.023, Fig. 1), but all-cause death was not different (log rank p = 0.613). In multivariate analysis, thrombolysis was predictor of cardiac death.
Conclusion : In our experience, surgical thrombectomy was related to lower cardiac death than thrombolysis. For a patient who does not have life-limiting severe comorbidity, surgical thrombectomy can be a first-line option for acute massive pulmonary embolism.
책임저자: 조양현
성균관대학교 의과대학 삼성서울병원 흉부외과학교실
연락처 : 조양현, Tel: 02-3410-2213 , E-mail : mdcho95@gmail.com
